Have you ever wondered what the purpose of even getting up and going to work is? Have you ever questioned the logic behind the way most people lead their lives: get a good job, marry, have kids?
Most people have asked themselves these questions at some point or another. That’s normal. Skepticism is healthy. It qualifies you as a thinking, rational being.
The problem is when those thoughts take over your life and impede your ability to enjoy and grow.
I remember searching for myself as a young adult. I did this the only way I knew: traveling around the world and trying new things. I thought, perhaps, that I would find an occupation that I felt truly passionate about, something that would make me feel truly connected and alive.
Like so many other lost young men, I took it upon myself to complete what’s perhaps the world’s best-known pilgrimage: el Camino de Santiago. It would give me time to think and figure things out, I thought.
One day, walking on my own as I traversed the never-ending plains of Castilla, a thought struck me:
I realized that nothing mattered, that neither I nor my work made any difference in the grand scheme of things.
As this thought dawned on me, I felt a cold sweat run down my face. My body stiffened, and all of a sudden, I stopped paying attention to the outside world.
I was having an existential crisis.
That was my first encounter with existential OCD. I would have many more during my walk and throughout my early twenties.
The problem was that the more I tried to think my way out of my mental cacophony, the more enmeshed I became in my obsession. The more I told myself that life had a purpose, the stronger the thought “life is meaningless” became.
I spent a lot of time throughout my journey thinking about this topic (I had plenty of time), and it only made it worse. By the time I reached the glorious Cathedral of Compostela, I was feeling truly awful and lost.
Now, recovery did not come easy. Like the pilgrimage itself, overcoming my existential OCD was a long journey, and it began with making some room for the uncertainty I was feeling around life’s purpose.
Once I accepted that uncertainty and those difficult thoughts and feelings, I stopped trying to problem-solve. This, in turn, gave me time back to focus on the things that I enjoyed and on the life that I wanted to lead.
As I was able to relax around this topic, the grip that this obsession had over me slowly weakened. Now, it almost feels like a distant nightmare.
What Is Existential OCD?
As you can infer from my story above, existential OCD is a particular thought pattern centered around life’s big questions, such as the purpose of existence and death. It is a common type of OCD. Check this article to learn more about OCD.
People with this OCD subtype may question the purpose of getting up in the morning. They may even question whether their life is real or if they are living in some kind of simulation.
What Makes Existential OCD Different From Normal Worry?
As with other types of OCD (such as false memory OCD or relationship OCD), the difference between regular reflection about life’s purpose and the type of rumination we see in existential OCD is that the latter is much more persistent and causes significantly more anxiety, doubt, and distress. If you want to know more about what OCD rumination looks like, check this article.
Likewise, people experiencing normal, occasional questioning do not typically engage in compulsions. By contrast, one of the defining characteristics of existential OCD is engaging in compulsive behavior.
Common Compulsions in Existential OCD
One of the reasons existential OCD can feel so overwhelming is that the mind is constantly trying to resolve these questions.
This often leads to compulsive behaviors, many of which are mental and therefore harder to recognize.
Some common compulsions include:
Mental rumination: Replaying the same questions over and over in an attempt to reach a satisfying answer.
Seeking certainty: Trying to arrive at a definitive conclusion about life’s meaning, reality, or existence.
Reassurance seeking: Asking others for their perspective or looking for answers in books, videos, or online forums.
Checking how you feel: Constantly monitoring whether things “feel real” or meaningful.
Avoidance: Staying away from topics, conversations, or environments that might trigger these thoughts.
While these behaviors may provide temporary relief, they tend to reinforce the cycle over time, making the thoughts come back stronger.
How Is Existential OCD Treated?
As counterintuitive as it may sound, the way out of existential OCD is not to solve the questions that your mind is presenting.
In fact, trying to find a final answer is often what keeps the cycle going.
A more effective approach involves changing your relationship with these thoughts.
This is where approaches like Acceptance and Commitment Therapy (ACT) can be helpful. Instead of trying to eliminate or resolve the thoughts, the focus shifts to:
Increasing your psychological flexibility so that you become more resilient and able to redirect your attention toward actions that align with your values.
Over time, as you reduce the amount of energy you give to these questions, they tend to lose their intensity and frequency.
This doesn’t mean the questions disappear entirely. It means they no longer control your life.
Creative hopelessness is the realization that our old control strategies don’t work because the pain that we are trying to avoid cannot be avoided. It leans on the sense of freedom that comes with accepting the pain that comes with being alive and the futility of trying to avoid it.
Once we accept that we cannot escape difficult experiences, we can stop fighting and use our energy instead for the things and activities that we value.
Creative hopelessness is about changing the way we relate to difficult thoughts and emotions, and it is an important element of enhancing psychological flexibility. It is about coming to terms with the fact that excessive control has not worked and will not work.
Instead, we need a new approach, one that forces us to think about our problems in completely different, more “creative” ways.
What Is Creative Hopelessness in ACT?
Creative hopelessness permeates many of the ideas that Acceptance and Commitment Therapy (ACT) is based on. Defusion and acceptance exercises, important elements of the ACT framework, aim to free us of the burden of unhelpful and unworkable control strategies. At the same time, ACT also emphasizes clarifying one’s values to lead a life that’s meaningful.
At its core, creative hopelessness is often the turning point in ACT. Before this point, much of our energy is spent trying to control, eliminate, or reduce unwanted thoughts and feelings. We analyze them, challenge them, suppress them, or try to outthink them.
In the short term, some of these strategies may provide relief. In the long term, however, they tend to reinforce the very patterns that keep us stuck. ACT gently brings this pattern into awareness. It asks a simple but uncomfortable question: Has this been working? Not in theory, but in your actual lived experience.
When the answer becomes clear, something shifts. This is not about giving up on feeling better. It is about giving up on strategies that, despite our best efforts, have not delivered the life we want. From there, ACT opens a different path, one based not on control, but on acceptance, presence, and values-based action.
Creative Hopelessness: A Practical Example
Picture this: you’ve just arrived at a new destination. It is a busy, bustling seaside city. It is full of life, full of distractions, and… full of noise. The problem is… you are very sensitive to noise.
Although you love the city’s vibrant personality, you feel a pang of anxiety every time a car zips past you while honking or when a kid screams at the top of their lungs for their mother.
You cope with these micro-shocks to your system with a never-ending array of strategies: you remind yourself that people in this country are more tolerant of noise than people in your country. You tell yourself that, actually, the noise doesn’t bother you at all.
However, every time you are startled by a noise, you feel the pang of anger rise within you, and you quickly feel the need to resort to one of the many control strategies you’ve been employing. And so it goes, without you even realizing it, you’re deploying a non-insignificant amount of resources to deal with these uncomfortable thoughts and emotions. Worst of all, it hasn’t helped one bit.
A bit downtrodden, you sit on a bench to ponder. And right then and there, you realize there is only one thing you haven’t done: accepting that the noise is there and that it will always be there, sometimes shocking you, sometimes mocking you like a willful bully. Instead of battling with it, you realize it makes more sense to focus on something that you value: the beauty of the chaos and of the way of being that unfolds in front of you.
What Is the Purpose of Creative Hopelessness?
The purpose of creative hopelessness is not to make you feel defeated. It is to help you see, clearly and honestly, that the strategies you have been relying on are not giving you the life you want.
In many cases, especially with OCD, these strategies are understandable. They are attempts to reduce anxiety, gain certainty, or protect yourself from harm. But over time, they tend to backfire. They consume your attention, reinforce doubt, and keep you stuck in repetitive cycles.
Creative hopelessness brings this pattern into focus. It helps you step back and ask: If this hasn’t worked so far, what am I holding on to?
This realization creates space. Space to stop investing energy in a losing struggle. Space to consider a different way of relating to your thoughts and emotions. And, most importantly, space to start moving toward what actually matters to you.
In that sense, creative hopelessness is not the end of the road. It is the beginning of a more workable one.
Creative Hopelessness Metaphors
Metaphors, like the paper prison, can be very useful to help us understand psychological concepts as they can feel a bit abstract. Here are a couple of metaphors often used to explain the concept of creative hopelessness.
The Chinese Finger Trap
The Chinese finger trap is a simple but powerful metaphor. When you place your fingers inside the trap and try to pull them out, the trap tightens. The harder you pull, the more stuck you become.
The only way to free yourself is to do the opposite of what your instincts tell you: you gently push your fingers inward, creating enough slack to release them.
In the same way, many of our control strategies tighten the grip of anxiety and intrusive thoughts. The more we try to escape them, the more entangled we become. Creative hopelessness is the moment we realize that pulling harder is not the solution and that a completely different approach is needed.
Tug of War
Imagine you are in a tug of war with a monster. On the other side of the rope is everything you fear: your intrusive thoughts, your anxiety, your doubts. Between you and the monster is a deep pit.
You pull with all your strength to avoid being dragged into the pit. The problem is, the monster pulls back just as hard. The struggle continues, exhausting and endless.
Creative hopelessness is the moment you realize that no matter how hard you pull, you cannot win this game. The only way out is to drop the rope.
Dropping the rope does not make the monster disappear. It simply ends the struggle. And in doing so, it frees you to step away from the pit and move in a different direction.
Creative Hopelessness: Final Thoughts
Creative hopelessness can feel uncomfortable at first. It asks you to question strategies that may have felt necessary, even protective, for a long time.
But there is something deeply liberating about seeing things as they are.
When you recognize that the struggle to control your inner experience is not working, you are no longer trapped in it in the same way. You can begin to loosen your grip, redirect your energy, and engage more fully with your life.
This is not about resignation. It is about honesty.
And from that honesty, a different kind of hope can emerge: one grounded not in eliminating discomfort, but in building a life that feels meaningful, even in its presence.
OCD rumination is a mental compulsion, not just overthinking.
It feels like problem-solving, but it is actually part of the OCD cycle that keeps anxiety alive.
The more you ruminate, the more uncertain you feel.
Rumination is driven by a need for certainty and a desire to get rid of anxiety but it has the opposite effect.
Recovery involves changing your response to thoughts, not eliminating them.
Approaches like ERP and ACT help you tolerate uncertainty and step out of the rumination loop.
Disclaimer: This article is for educational purposes, not medical advice.
OCD Rumination Explained
Rumination is not just “thinking too much.” It is a mental process where you try to solve, analyze, or get certainty about something that feels unresolved.
In OCD, rumination becomes a mental compulsion. It is an attempt to reduce anxiety, doubt, or discomfort by thinking things through again and again. Unlike visible compulsions, such as checking or washing, this happens entirely in your head, which makes it harder to notice.
OCD rumination often feels productive at first. It can seem like you are being responsible, careful, or thoughtful. But in reality, you are stuck in a loop of obsessive thinking that does not lead to resolution.
Rumination is also not unique to OCD. It appears in other conditions such as ADHD, anxiety, and depression. The key difference is that in OCD, it is driven by a need for certainty and relief from intrusive thoughts.
What Does OCD Rumination Feel Like?
If you have experienced OCD rumination, you will likely recognize the pattern immediately. It has a very specific “texture” in the mind.
Common traits include:
Repetitive thoughts that feel impossible to settle.
Distressing mental loops that create anxiety.
A sense that the thinking is involuntary or hard to stop.
An urge to resolve doubt or reach certainty.
Going in circles without reaching a clear answer.
Constant reviewing, analyzing, or replaying situations.
OCD rumination is not just thinking. It feels urgent. It feels like something needs to be figured out right now.
At the same time, there is a subtle awareness that the process is not helping. You may notice that no matter how much you think, the relief never lasts.
Is OCD Rumination the Same as Overthinking?
It is easy to confuse OCD rumination with overthinking, but they are not the same.
Overthinking can happen to anyone. It might involve worrying about decisions, replaying conversations, or imagining future scenarios. While uncomfortable, it is usually flexible and can stop when attention shifts.
OCD rumination is different. It is compulsive
It is driven by anxiety and the need to eliminate uncertainty. The thinking feels necessary, almost like a responsibility. You may believe that if you do not fully think something through, something bad could happen or you could be making a serious mistake.
Another key difference is that OCD rumination tends to get stronger the more you engage with it. Instead of resolving the issue, it reinforces the cycle.
OCD Rumination
Overthinking
Driven by anxiety and a need for certainty
Often driven by stress, curiosity, or decision-making
Focused on resolving doubt or preventing something bad
Focused on evaluating options or reflecting on situations
Repetitive and circular, going over the same thoughts again and again
Can move between different ideas or scenarios
Gets stronger the more you engage with it
Usually fades when attention shifts
Does not lead to resolution or relief long-term
Can sometimes lead to decisions or insights
Reinforces the OCD cycle
Does not typically create a self-perpetuating cycle
Examples of Rumination in OCD
To better understand OCD rumination examples, it helps to look at how it shows up in different themes.
Relationship OCD
Daniel finds himself constantly analyzing his feelings toward his partner, which is a common OCD pattern known as Relationship OCD.
“Do I really love them?” “What if I am lying to myself?” “What if I am wasting their time?”
At first, it starts as a passing doubt. One evening, he notices he does not feel as connected as usual, or he catches himself comparing his relationship to someone else’s. The thought lingers longer than it should, and instead of letting it pass, his mind locks onto it.
He begins replaying conversations, searching for clues. Did I feel enough when they said “I love you”? Did I hesitate? Should I have felt something stronger? He studies their expressions, their tone, even small pauses, trying to extract certainty from each interaction.
The analysis spreads into everything. He compares his relationship to others, to movies, to past experiences. He tries to measure his feelings, hoping to reach a clear answer. But each time he gets close, a new doubt appears.
“What if I am just convincing myself?” “What if I am missing something important?”
The more Daniel thinks, the less certain he feels. What once felt natural now feels forced and examined. Instead of being present in the relationship, he is stuck evaluating it, trapped in a loop that never quite resolves.
Harm OCD
María is washing dishes when an intrusive thought flashes through her mind. It is sudden and disturbing, completely out of line with who she believes herself to be. It involves harming a loved one, which is a common fear among people with Harm OCD.
For a moment, she freezes. Then the questioning begins.
Why would I think that? Does this say something about me? She tries to trace the thought back to its origin, searching for a reason that would make it feel less threatening. Maybe it was stress. Maybe she is just tired. But the explanations never feel convincing enough.
She starts reviewing her past. Has she ever acted aggressively? Has she ever come close to losing control? She replays memories, analyzing her intentions in each one, looking for proof that she is safe.
For brief moments, she feels relief. She tells herself she would never act on such a thought. But then doubt creeps back in.
“What if I am missing something?”
“What if this time is different?”
The urgency builds, pulling her back into the same mental loop. The more María tries to prove to herself that she is not dangerous, the more real the fear begins to feel. The process feels necessary, even responsible, but it never fully resolves the anxiety.
Real Event OCD
Lucas is traveling through China as part of a university program. One afternoon, he rents a bike with a couple of classmates and heads out for a ride near Guilin. As he cycles down a quiet road, he notices a young girl standing off to the side. He does not get a clear look at her, just a brief impression as he passes.
A thought appears. Is she okay? Does she need help?
He considers stopping, but his classmates are already ahead. If he stops, he might lose them. So he keeps going.
Later, back at the hotel, everyone is relaxed and talking. But Lucas is stuck on that moment. He begins replaying it in his head, trying to reconstruct what he saw. With each replay, the image changes slightly. Now she looks more distressed. Now she seems disheveled. Now it feels like something was clearly wrong.
The doubt grows heavier. What if she needed help and I ignored her? What if something bad happened because I didn’t act?
He spends hours going over the scene, analyzing every detail, trying to reach certainty. He tells himself that he will go back the next morning and find her. This is a classic example of Real Event OCD where the more he thinks about the issue, the more uncertain he becomes.
Real Event OCD involves things that have actually happened, but the mind gets stuck analyzing, doubting, or morally judging the event far beyond what is helpful. A similar OCD theme is False Memory OCD, where the person worries that something bad may have happened despite little or no clear evidence.
How to Stop OCD Rumination
It is not easy to stop ruminating, particularly if you are a person that has been diagnosed with OCD. The first step in stopping OCD rumination involves understanding something counterintuitive:
Rumination does not solve the problem. It only reinforces the OCD cycle
We ruminate because we believe it is a workable way to end the obsession and get rid of the anxiety. It makes sense to us that if we think hard enough, we’d be able to “solve” the issue. In reality, OCD obsessions cannot be resolved through logic or brute force, and rumination only help reinforce the vicious mental pattern known as the OCD cycle.
This cycle is simple:
An obsession creates anxiety
To placate the anxiety, we ruminate
Rumination leads to short-term relief
The obsession reappears because we did not solve the issue, which cannot be solved to begin with, and the cycle starts again
To escape the cycle, we need to let go of the notion that we need to “figure it out.” Instead, we first need to understand that ruminating doesn’t solve the problem. The next step is to become aware of the fact that we are ruminating. Only once we realize we are ruminating are we able to change this behavior.
ERP (Exposure and Response Prevention)
ERP is one of the most effective treatments for OCD and is a specific form of Cognitive Behavioral Therapy. It directly targets the cycle that keeps OCD going, which includes both obsessions and compulsions like rumination.
The key idea is response prevention, not thought suppression. You are not trying to get rid of the thought or prove it wrong, but rather to stop responding to it with compulsive thinking.
You allow the intrusive thought or doubt to be there without engaging in rumination. This means resisting the urge to analyze, solve, or mentally review, even when it feels uncomfortable or irresponsible to do so.
At first, this can feel very counterintuitive. Your mind will tell you that you need to figure it out, that this time is different, or that ignoring it could have consequences.
Over time, your brain learns that the anxiety can rise and fall on its own. When you stop feeding the cycle, the urgency of the thoughts begins to decrease, even if the thoughts themselves still appear.
This builds tolerance for uncertainty, which is at the core of OCD recovery. Instead of needing answers, you learn that you can handle not knowing, and that is what ultimately breaks the grip of rumination.
ACT (Acceptance and Commitment Therapy)
ACT takes a slightly different approach but complements ERP well. It focuses less on reducing symptoms directly and more on changing your relationship with your thoughts.
Instead of trying to control your thoughts, ACT focuses on building psychological flexibility. This means being able to experience difficult thoughts and feelings without getting stuck in them or letting them dictate your actions.
In practice, this means learning to notice thoughts without getting pulled into them. A ruminative thought can show up, and instead of analyzing it, you acknowledge it and allow it to pass without engaging.
For example, instead of getting caught in a loop of doubt, you might gently redirect your attention to a meaningful activity, even while the uncertainty is still present. The thought does not need to be resolved for you to move forward.
Over time, this creates space between you and your thoughts. You begin to see that thoughts are not commands or problems that must be solved, but mental events that come and go.
The goal is not to feel certain. The goal is to live well alongside uncertainty, guided by your values rather than by the need to eliminate doubt.
Medication
In some cases, medication can help reduce the intensity of OCD symptoms, including rumination.
Selective serotonin reuptake inhibitors, often called SSRIs, are commonly prescribed. They can make it easier to disengage from compulsive thinking and participate in therapy.
Medication is not a standalone solution for most people, but it can be a helpful support when combined with approaches like ERP or ACT.
Final Thoughts
OCD rumination is one of the most misunderstood parts of the condition. Because it happens internally, it can feel like “just thinking,” when in reality it is a powerful compulsion.
If you take one thing from this, let it be this:
You do not need to solve your thoughts.
The more you try to think your way out of OCD, the more stuck you become. Recovery begins when you step out of the loop, not when you win the argument in your head.
Rumination OCD FAQ
How do you overcome rumination OCD?
Overcoming rumination OCD involves recognizing rumination as a compulsion and resisting it. Approaches like ERP and ACT help you tolerate uncertainty without engaging in repetitive thinking.
What are the best apps for managing rumination OCD symptoms?
Apps like NOCD, GG OCD, and mindfulness apps can support recovery by guiding ERP exercises, building awareness, and helping you disengage from rumination and compulsive thinking.
How do you ignore OCD compulsions?
You do not ignore compulsions by force. Instead, you notice the urge and choose not to engage with it, allowing anxiety to rise and fall without performing the compulsion.
What is the 3 3 3 rule for OCD?
The 3-3-3 rule is a grounding technique where you name three things you see, hear, and feel. It can help shift attention away from rumination temporarily.
ADHD and OCD can look similar on the surface, but they are driven by very different mechanisms: impulsivity and attention dysregulation vs anxiety and compulsions.
Both conditions affect executive functioning, which is why they are often confused or misdiagnosed, especially in children.
ADHD and OCD can co-occur, but true dual diagnosis appears less common in adults than in children.
Effective treatment depends on accurate diagnosis, as approaches differ significantly and some ADHD treatments may worsen OCD symptoms.
Disclaimer: This article is for educational purposes, not medical advice.
OCD vs ADHD: Understanding the Key Differences
At first glance, Attention-Deficit/Hyperactivity Disorder (ADHD) and Obsessive-Compulsive Disorder (OCD) can look surprisingly similar. Both can affect attention, focus, and daily functioning. Both often begin in childhood. And both are linked to difficulties with executive functioning.
But beneath the surface, they are very different conditions.
One helpful way to understand ADHD vs OCD is through the idea of externalizing vs internalizing disorders. ADHD is an externalizing disorder. It affects how a person interacts outwardly with their environment, often leading to impulsivity and risk-taking.
OCD, on the other hand, is an internalizing disorder. It involves turning inward, with intrusive thoughts and compulsive behaviors aimed at reducing anxiety.
Another way to contextualize this is to think of these disorders as part of the same continuum, the compulsive-impulsive continuum. OCD sits on the compulsive end, while ADHD sits on the impulsive end.
This difference shows up clearly in behavior. People with ADHD tend to be more impulsive and novelty-seeking. People with OCD tend to be more cautious, introspective, and risk-averse.
ADHD and OCD involve the same brain circuit, the frontostriatal system, but in opposite ways. ADHD is associated with underactivity, while OCD is linked to overactivity.
What Is ADHD?
ADHD is a neurodevelopmental condition characterized by persistent patterns of inattention, hyperactivity, and impulsivity. It is fundamentally about difficulty regulating attention, especially when tasks are not engaging.
ADHD is one of the most common psychiatric conditions in children. A large global study from 2007 estimated that ADHD affects about 5.2% of children and adolescents worldwide.
ADHD Symptoms and Behavior
ADHD is generally categorized into three presentations: predominantly inattentive, predominantly hyperactive-impulsive, and combined. These presentations describe which symptoms are most prominent, although they can change over time as a person develops.
Behaviors associated with predominantly inattentive ADHD include:
Difficulty focusing or staying on task.
Easily distracted by external stimuli.
Forgetfulness and disorganization.
Trouble following through on tasks.
Behaviors associated with predominantly hyperactive-impulsive ADHD include:
Restlessness and difficulty sitting still.
Talking excessively or interrupting others.
Acting without thinking.
Seeking stimulation or novelty.
What Is OCD?
OCD is a mental health condition characterized by a cycle of obsessions and compulsions. People with OCD often experience intrusive thoughts that cause anxiety and disrupt their lives. To cope with this anxiety, they often engage in compulsions.
OCD Obsessions and Compulsions
Obsessions are intrusive, unwanted thoughts, images, or urges that create anxiety or distress. In OCD, obsessions tend to be ego-dystonic, meaning that they are in conflict with the values of the person. For example, a person who cares deeply about their romantic relationship may experience intrusive thoughts about their partner not being “the one,” commonly known as relationship OCD.
Compulsions are behaviors or mental acts performed to reduce that anxiety. However, compulsions don’t work. While they may provide temporary relief, the anxiety or obsession always comes back stronger.
Examples of common compulsions include:
Checking.
Cleaning.
Reassurance seeking.
Repeating actions.
ADHD vs OCD: Key Differences
When comparing ADHD vs OCD, the differences become clearer:
Core motivation: ADHD is driven by difficulty regulating attention and impulses. OCD is driven by anxiety and the need to reduce uncertainty.
Impulsivity vs compulsivity: ADHD involves impulsive behavior, while OCD involves repetitive, rule-based behavior.
Risk profile: ADHD is associated with risk-taking. OCD, on the other hand, is associated with risk avoidance.
Attention problems: ADHD attention is pulled outward by distractions. People with OCD, meanwhile, find their attention is pulled inward by intrusive thoughts.
Behavior patterns: ADHD tends to be associated with disorganization, while OCD is often characterized by rigidity and excessive structure.
OCD and ADHD Overlap: Why They Can Look Similar
Even though the brain activity patterns differ in both conditions, both OCD and ADHD are associated with deficits in executive functioning, including planning, working memory, and response inhibition.
Due to these deficits in executive functioning, people with OCD or ADHD, or both, may struggle with focus, task completion, and organization.
There is also the idea of executive overload. In OCD, intrusive thoughts can overwhelm the brain’s capacity, making it difficult to focus on external tasks. This can make OCD look like ADHD, especially in children. Because of this overlap, ADHD and OCD are often misdiagnosed.
Can You Have ADHD and OCD Together?
While the common answer is “yes,” the picture is complex. According to the International OCD Foundation, results are inconsistent, with research showing a wide range of co-occurrence rates, from 0% to 59%.
For example, a 2006 study examined 94 children and adolescents diagnosed with OCD and found that over 25% of children and 17% of adolescents also had ADHD. Another study from 2010 reported a co-occurrence rate of 11.8%.
The International OCD Foundation says that 21% of children with OCD also have ADHD. For adults, the figure drops to 8.5%.
Meanwhile, a study from 2014 that assessed the neurobiological link between OCD and ADHD found that “ADHD was the most common comorbidity in early-onset OCD, in which tic and Tourette syndrome were exclusion criteria.”
However, the International OCD Foundation suspects that “full-blown dual diagnosis of ADHD and OCD in adults is in fact rather rare,” adding that ADHD-like symptoms in children with OCD may actually stem from OCD itself. As the brain develops, these symptoms may change or disappear.
Are OCD and ADHD Often Misdiagnosed?
Yes, OCD and ADHD are often misdiagnosed, largely because they can look similar on the surface. In both conditions, a person may appear distracted, unfocused, or disengaged. However, the underlying reasons for this distraction are very different.
In ADHD, attention is typically pulled outward by external stimuli. The person may struggle to stay focused because their mind is constantly shifting from one thing to another. In OCD, attention is pulled inward. The person may appear distracted because they are preoccupied with intrusive thoughts, doubts, or mental rituals.
Because both conditions involve difficulties with attention and executive functioning, clinicians may mistake one for the other. In some cases, OCD is misdiagnosed as ADHD. In others, one condition is identified while the other is overlooked entirely.
This is especially common in children, where diagnosis often relies on observations from parents and teachers. A child with OCD may seem inattentive in class, but the issue is not a lack of focus in the traditional sense. Instead, their attention is consumed by internal thoughts, such as worries, fears, or the need to mentally review something.
This is why understanding the difference between ADHD and OCD is so important. Without a clear distinction, the underlying problem can be misunderstood, leading to ineffective or even counterproductive treatment.
How OCD and ADHD Are Diagnosed
The diagnostic process for both OCD and ADHD typically involves a structured clinical assessment rather than a single test. Clinicians use standardized criteria, such as those outlined in diagnostic manuals, along with symptom checklists, interviews, and reports from the individual and, in the case of children, from parents or teachers.
The goal is to understand not just what behaviors are present, but why they are happening and how they impact daily functioning across different settings.
The International OCD Foundation recommends that clinicians pay close attention to two key factors when distinguishing between OCD and ADHD. The first is the presence of impulsivity and risk-taking. These traits are strongly associated with ADHD.
The second factor is the ability to perform detailed, repetitive behaviors that follow strict and often complex rules. This is a hallmark of OCD. People with ADHD, on the other hand, tend to struggle with sustained attention and consistency, making it difficult to follow through on complex, rule-based routines.
Ultimately, accurate diagnosis depends on understanding the underlying motivation behind the behavior. What may look similar on the surface can have very different causes, which is why a careful and thorough assessment is essential.
Causes of OCD and ADHD
Both ADHD and OCD arise from a combination of genetic, neurological, and environmental factors.
They involve the same brain circuit, the frontostriatal system, but in different ways. In ADHD, this circuit tends to be underactive, while in OCD it is overactive, leading to very different patterns of behavior.
The two conditions also involve different neurotransmitters. ADHD is primarily linked to dopamine, which affects motivation and attention, whereas OCD is more closely associated with serotonin, which plays a role in mood and anxiety regulation.
Treatment of ADHD and OCD
Treatment differs depending on the condition, although there can be some overlap in approaches.
For OCD, the most effective treatment is Exposure and Response Prevention (ERP), a form of Cognitive Behavioral Therapy (CBT) that helps individuals gradually face their fears without engaging in compulsions.
CBT more broadly can help challenge unhelpful thinking patterns, while Acceptance and Commitment Therapy (ACT) focuses on building psychological flexibility and changing the relationship to intrusive thoughts. In some cases, medication such as SSRIs may also be prescribed to help reduce the intensity of symptoms.
For ADHD, treatment typically focuses on improving attention, organization, and impulse control. This may include behavioral strategies, skills training for time management and focus, and medication, either stimulant or non-stimulant, depending on the individual’s needs.
When ADHD and OCD occur together, treatment becomes more complex and needs to be carefully balanced. For example, stimulant medication used for ADHD may sometimes worsen OCD symptoms in certain individuals. For this reason, it is important that treatment is guided by a clinician who can monitor symptoms closely and adjust the approach accordingly.
ADHD vs OCD FAQ
Which is worse, ADHD or OCD?
Neither ADHD nor OCD is inherently “worse.” Both can significantly impact daily life in different ways. OCD often involves intense anxiety and distress, while ADHD affects attention and impulse control. Severity depends on the individual and how symptoms interfere with functioning.
What is the difference in testing for OCD vs ADHD?
Both are diagnosed through clinical assessments, not lab tests. ADHD evaluation focuses on attention, impulsivity, and behavior across settings. OCD assessment focuses on intrusive thoughts and compulsions, including their frequency, distress, and impact on daily life.
What medication options are available for managing ADHD vs OCD?
ADHD is commonly treated with stimulant or non-stimulant medications that target attention and impulse control. OCD is typically treated with SSRIs, which help regulate anxiety. Medication choice depends on symptoms and should be guided by a qualified clinician.
Where can I find a specialist able to differentiate ADHD from OCD?
Look for licensed psychologists or psychiatrists with experience in both ADHD and OCD. Specialists in anxiety disorders or neurodevelopmental conditions are ideal. Reputable directories, such as professional associations or mental health organizations, can help you find qualified providers.
When it comes to Obsessive-Compulsive Disorder (OCD), there is a lot of confusion. Most laypeople believe it is simply being very particular about how you organize your things.
Those somewhat more familiar with psychology may equate the condition with a compulsive need to perform repetitive actions, such as washing hands.
The truth is that it is those things… and much, much more.
OCD is less about a single behavior and more about a set of recurring mental patterns. Drawing from my own experience, I believe the “OCD mindset” is composed of the following elements:
An aversion to uncertainty.
A need for control.
The feeling that something is not quite right.
Taking responsibility for things beyond your control.
The content of your obsessions may change, but these elements are almost always present.
OCD likely has a genetic component, but it often lies dormant until triggered by a traumatic life event. In my case, that was the passing away of my father when I was around 12 years old.
My OCD started then, but it has since taken on many forms. My battle with OCD has often felt like an arms race. As soon as I learned to be okay with one particular theme, it would metamorphose into something new, usually something I had never seen or heard about before.
In this post, I would like to give you a tour of my OCD, from its more rudimentary beginnings to the increasingly complex and sophisticated forms it has taken over the years. I hope it helps demystify the condition for non-sufferers and helps others feel less alone in their experience.
The Quest for Balance: Just-Right OCD
The summer in which my father died, something shifted in me. It was as if there had been a big red button inside my head my whole life. It had always been there, dormant, until the tiny, mischievous gremlin that lives between the folds of my brain decided to push it.
When that button was pushed, a very well-defined feeling of incompleteness, of something not quite right, crept into my awareness. And it wasn’t abstract. It attached itself to something very concrete in the real world.
In this case, it was a small patch of dirt in the garden where we kept a little farm.
What exactly was wrong with that patch of dirt, I could not tell you. But I was certain that something about it was off, even though no one else in the world would have noticed it.
The first day this feeling appeared, I dealt with it pragmatically: I tried to fix the patch of dirt with my own two hands. Delicately and diligently, almost like an artist shaping a new creation, I nudged and pushed the soil here and there until it felt right.
I spent maybe five or ten minutes working on it and then left. I wasn’t totally satisfied, but I figured I would eventually forget about it.
I didn’t.
The next day, I woke up with the same nagging feeling. I went back to try to fix it again, but this time I spent longer, perhaps twenty minutes. As I worked on this thankless crusade for balance, I grew more and more frustrated. It would never be right.
That same day, I returned in the afternoon and spent another ten or fifteen minutes trying to fix it, trying to achieve this imaginary sense of balance. When I was done, I went back inside, only to find that I was still thinking about it, still trying to solve it in my head.
And just like that, something small and insignificant, something no one else would have noticed, began to take up more and more space in my mind.
Control Through Rituals: Magical Thinking OCD
The whole ordeal with the patch of dirt lasted a couple of weeks. Eventually, I was able to stop myself from going back to the garden, and the obsession gradually faded.
But almost immediately, something else took its place.
One evening, as I was getting ready for bed, I had the strange feeling that I needed to do something very precise in order to fall asleep. I needed to open and close the wardrobe exactly three times, and each repetition had to feel right. If anything felt even slightly off, I had to start again from the beginning.
That evening, I gave in to the urge. When I was finished, I felt a sense of relief and went to bed.
The next night, I tried to go to sleep normally, but I couldn’t. I needed to perform the wardrobe ritual again. Otherwise, I feared, I wouldn’t be able to sleep at all.
I stood in front of the wardrobe and carried out the ritual. This time, it took longer. I had to repeat several sets, each consisting of opening and closing the door three times.
Even after finishing, I still felt like I hadn’t done it quite right. A sense of dread began to grow inside me as I realized that something very important was at stake: my sleep.
Sleep, I had always been told, was essential. I needed at least eight hours to function well, to perform at school, to get good grades. It wasn’t optional. It was necessary.
Looking back, what was happening is clear. Because of my rigid beliefs about sleep, I developed a compulsion that actually made it harder for me to sleep. I was trying to control sleep, and the only way my mind found to do that was through this ritual.
This went on for months. During that time, I got very little sleep. Some nights, I didn’t sleep at all. I would lie in bed with my eyes wide open, watching the sun rise, filled with dread at the thought of facing another long day of school without rest.
The whole ordeal ended in a surprising way. One day, I realized that it had been months since I had slept properly… and yet I hadn’t missed a single day of school, and my grades were fine.
It dawned on me that perhaps sleep wasn’t as important as I thought. As I loosened my rigid beliefs around sleep, something changed. That very same night, I slept like a baby.
Putting the Weight of the World on My Shoulders: Real Event OCD
Fast forward several years. I am now a university student, traveling through East Asia with classmates and professors as part of a special program. We are near Guilin, in China, and a couple of friends and I decide to rent bikes and go for a ride.
As I ride, I notice a young girl by the side of the road. She is maybe eight or nine, though I don’t get a good look at her.
A thought appears: Is she okay? Does she need help?
I consider stopping, but my classmates are already ahead of me. If I stop, I’ll lose them. So I keep going.
We return to the hotel. Everyone is chatting and enjoying themselves, but I am somewhere else entirely. I am stuck on that moment.
I begin replaying the scene over and over. With each replay, more details emerge. Now she looks disheveled. Now she seems distressed. I start to convince myself that she is in urgent need of help, that something terrible will happen if I don’t intervene.
That evening, I spend hours trapped in these thoughts. The more I think, the more anxious I become. I tell myself that the next morning I will go back and find her.
I never do.
Eventually, I tell myself it’s too late, that she won’t be there anymore. Slowly, I calm down and fall asleep.
Looking back, it is clear that this episode was driven by an inflated sense of responsibility, a common feature of OCD. This experience could be classified as real event OCD: I experienced something ambiguous, and my mind filled in the gaps in the worst possible way. The more I obsessed, the more real and urgent the situation felt.
The Fear of Uncertainty: Relationship OCD
Fast forward again. I am now in my 30s and in a serious relationship.
Before we started dating, we had been good friends for over a year. We got along well, shared similar values, and saw the world in similar ways. When we eventually moved in together, it felt natural.
On the surface, everything was great. We were both growing, both professionally and personally, and everyone thought we made a great couple.
But inside my head, things were different.
A small voice was always there, whispering: Yes… but is she the one? Is there someone better out there for me?
That voice never left. It was there during quiet evenings, during time with friends, during conversations about our future.
Every few months, the tension would build to the point where I felt I had to do something about it. I would sit her down and tell her that something didn’t feel right, that although I loved her, I wasn’t sure.
She would respond with understanding. She would say that, although she wasn’t entirely sure I was the man of her life either, she still believed in the relationship. She would tell me that I made her life better, that we improved each other’s lives. And then, almost inevitably, she would start to cry.
After these conversations, I felt relief. The doubt and the guilt would temporarily fade. After all, if she wasn’t 100 percent sure either, then I wasn’t doing anything wrong by continuing the relationship.
But the doubt and the guilt always came back.
This was a textbook example of relationship OCD. I was unable to tolerate the uncertainty of not knowing whether she was “the one.”
What I regret most is how many moments I missed: moments where I could have been present with her but instead was trapped in my own mind, trying to resolve an unanswerable question.
What If I’m Dangerous: Harm OCD & False Memory OCD
Another theme that has come up repeatedly in my adult life is the fear that I might hurt people in the future, or that I have already done something terrible.
OCD often targets the things we care about most, generating intrusive thoughts that feel shocking precisely because they are so deeply at odds with our values. In fact, the more you value something (like being kind, safe, and responsible) the more OCD can latch onto it.
Let’s start with an example that is difficult for me to share, but one I’m including because I know how isolating these thoughts can be for people with OCD.
I have always felt comfortable around children, and I’ve always enjoyed spending time with them in a normal, caring way. One day, while I was playing with a group of children, a little girl sat on my lap. Almost immediately, an intrusive thought entered my mind: What if I get aroused?
The thought horrified me. I did not want it, and I did not agree with it, but once it appeared, I couldn’t stop monitoring myself. That evening, I became consumed by doubt. Had I gotten aroused? What would that mean about me? What if I were a danger to children?
From there, the obsession took on a life of its own, becoming a textbox example of false memory OCD. I replayed the moment over and over, searching for certainty, for proof, for some definitive answer that would relieve me of the fear. But like so many OCD spirals, the more I analyzed it, the worse it became.
After a few weeks of rumination, I spoke with people close to me and with my therapist, which helped. Even so, for a long time afterward, I avoided being around children altogether, just in case.
What made this experience so distressing was not any real desire or intention, but the meaning I attached to the thought. OCD had taken something I valued (being a safe, caring person) and turned it into a source of terror.
A few years later, I developed the obsession that I might harm people close to me, like my girlfriend or my sister. This is classic harm OCD.
I would scan my thoughts in search of anything that could be interpreted as dangerous: did I just wish this person would die? Did I imagine myself hurting them?
At the same time, I would spend hours trying to reason with myself, explaining why these thoughts didn’t mean I was a cold-blooded killer. The energy spent on these compulsions left little space for anything else.
This was the obsession that broke the camel’s back. It was at this point that I decided to talk to a therapist.
I was quickly diagnosed with OCD and given some very helpful guidance on how to relate to these thoughts. I began to understand that the reason they affected me so deeply was because I treated them as meaningful.
With time, I learned to see them for what they are: thoughts, random mental events that don’t require a response.
I started allowing them to be there without trying to solve them. And gradually, their weight began to fade.
I stopped ruminating and rationalizing. I no longer felt the need to. Thoughts are just thoughts.
And that, broadly speaking, covers the main OCD themes I’ve experienced. Within each, there were many more obsessions than the ones described here, but there isn’t space to go into all of them.
Reliving these experiences has been difficult, and I truly hope that someone can benefit from this. If you see yourself reflected in any of these situations, perhaps this can serve as a reminder: you are not a horrible person, but someone with a very tricky mind, one that targets what you care about most.
OCD is a complicated condition. It feeds on uncertainty and thrives on the illusion that we must control what lies beyond our reach.
One final note about what OCD is like. Sometimes, as an adult, I get flashbacks to a scene from my childhood. I must be three or four years old, sitting on the floor of my room, playing with my toys.
For some reason, I am alone.
I feel drawn to the wardrobe behind me. I don’t know what’s inside, but I’m sure it is something dark, something that could swallow me whole like a black hole.
I don’t know whether this memory happened exactly as I remember it, or why it has stayed with me so vividly. But over time, I have come to see whatever was inside that wardrobe as a representation of my OCD.
It is always there, trying to pull me in. And if I let it, it can take me away from the things that matter most.
Now, as back then, I have a choice: I can turn toward it, open the door, and get lost inside it. Or I can walk away and return to what actually matters: my family, my friends, life
False memory OCD is a form of obsessive-compulsive disorder in which a person becomes consumed by doubts about whether something happened in the past. These doubts often involve fears of having done something immoral, embarrassing, or harmful.
Unlike ordinary uncertainty about memory, false memory OCD creates intense anxiety and a powerful urge to “figure out the truth.” The more a person analyzes the memory, the more convincing the imagined scenario can become.
These doubts can feel incredibly convincing. A person may mentally replay a situation over and over, trying to determine whether something actually happened. Instead of gaining clarity, this repeated analysis often creates even more confusion and anxiety.
False memory OCD is closely related to real event OCD, another subtype where the focus is on something that actually happened in the past but becomes exaggerated or distorted by obsessive rumination.
This pattern is sometimes called blackout OCD, especially when someone fears they may have behaved badly during a time when their memory is unclear, such as after drinking alcohol. In these cases, the uncertainty becomes the fuel for obsessive doubt.
What Causes False Memory OCD?
Although not as common as other OCD subtypes, like harm OCD, false memory OCD is not rare. According to a study by NOCD, nearly 32% of people with OCD reported experiencing false memory OCD in 2023.
There is no single cause of false memory OCD. Like other forms of obsessive-compulsive disorder, it usually develops from a combination of the following factors:
Biological factors: Some people may have a genetic or family history of OCD, which can increase vulnerability. Differences in brain structure and functioning, particularly in areas related to threat detection and error monitoring, may also play a role.
Psychological factors: Certain cognitive patterns are also common in OCD. These include perfectionism, thought-action fusion, and heightened concern about morality. When these tendencies combine with uncertainty about memory, obsessive doubt can take hold.
Environmental factors: Life experiences can contribute as well. Traumatic events, stressful life transitions, or environments with strong moral expectations may increase sensitivity to intrusive thoughts.
Actual Example of False Memory OCD
Someone recently posted the following question on Reddit:
**“People with false memory—how can you tell?
Genuinely, how have people learned to tell the difference between a fact and a false memory? I find I almost create false memories in the moment, then question myself & my thoughts about it (i.e., but you thought about it so maybe you did it). I don’t know how to break this cycle because the imagery in my head is just so accurate & makes me feel as if I did the very thing I was avoiding not to do.
Thank you in advance, I’m just feeling really hopeless.”**
This post illustrates several key elements of false memory OCD.
First, the person describes intrusive imagery that feels extremely vivid. In OCD, imagined scenarios can become so detailed that they begin to feel like real memories. The brain fills in missing details, which makes the thought feel more convincing.
Second, the person is trapped in a loop of doubt and rumination. They try to determine whether the memory is real by analyzing their thoughts. But each attempt to figure it out only creates more uncertainty.
Third, the post highlights a common cognitive distortion in OCD: “If I thought about it, maybe I did it.” This reflects a pattern known as thought-action fusion, where the mere presence of a thought feels morally equivalent to having acted on it.
Importantly, the core problem here is not the memory itself. The real issue is the OCD-driven need for certainty about the past.
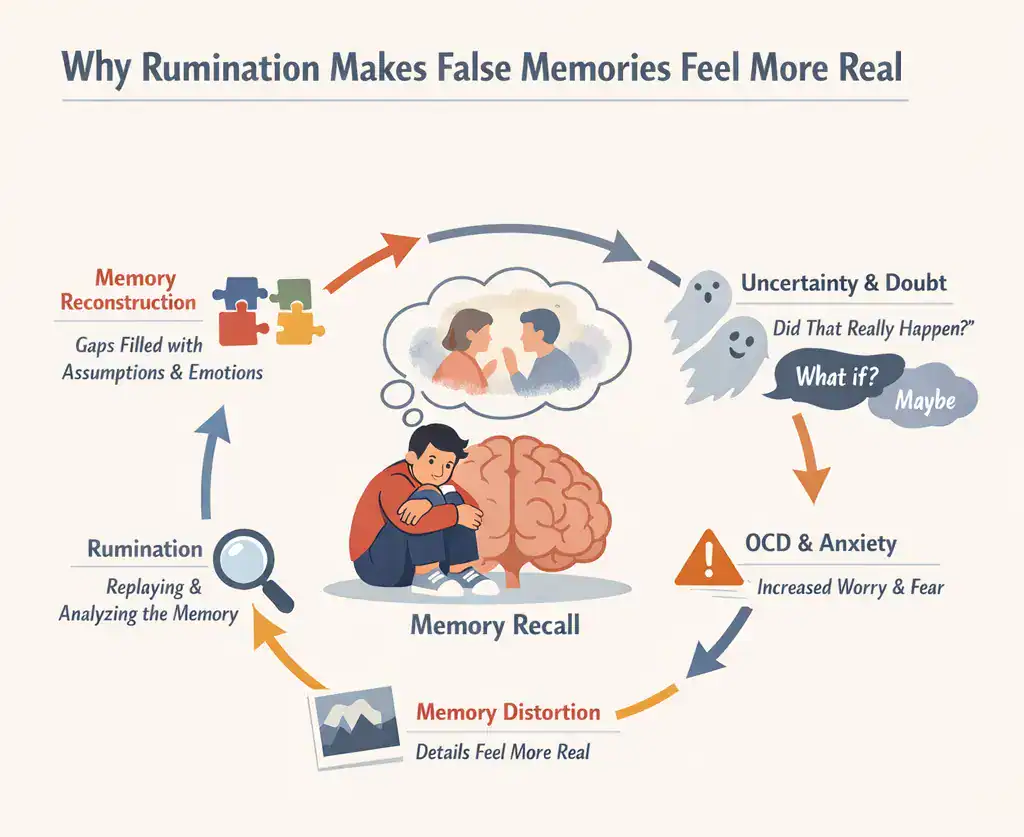
How False Memory OCD Work: The Role of Memory and Uncertainty
To understand false memory OCD, it helps to understand how memory actually works.
Many people assume that memory functions like a video recording that can be replayed with perfect accuracy. In reality, memory is reconstructive, meaning the brain rebuilds memories each time we recall them.
During recall, memories can become temporarily flexible in a process known as reconsolidation. This means details can be modified, strengthened, or altered with each recall. Because of this malleability, memory is far from perfect. The brain often fills in gaps using assumptions, emotions, and contextual cues.
In people with OCD, this normal imperfection can become a major source of anxiety. If someone already struggles with doubt, uncertainty about memory can feel intolerable.
Research supports this pattern. A study published in Psychological Medicine found that people with OCD tend to be less confident in their memory and perception than they should be, suggesting a genuine under-confidence in this population.
When a person begins analyzing a memory repeatedly, anxiety increases. That anxiety makes the memory feel more emotionally significant, which can strengthen imagined details. Rumination then reinforces the cycle.
The more someone mentally reviews the event, the more distorted and uncertain the memory becomes. This creates the central paradox of false memory OCD: the harder someone tries to verify the memory, the less certain they feel.
Difference Between Ordinary Memory Uncertainty and False Memory OCD
Everyone occasionally questions their memory. In false memory OCD, however, the level of doubt becomes persistent, distressing, and compulsive.
Ordinary Memory Uncertainty
False Memory OCD
Brief uncertainty about what happened
Persistent and intrusive doubts
Accepts ambiguity
Seeks absolute certainty
Moves on quickly
Replays the memory repeatedly
Little emotional distress
Intense guilt, anxiety, or shame
Common Examples of False Memory OCD
False memory OCD can focus on many different types of situations.
Common examples include:
Fear of having committed a crime, such as hitting someone with a car without realizing it.
Worry about having behaved inappropriately at a party.
Doubts about cheating on a partner or acting unfaithfully.
Fear of having harmed someone accidentally.
Worries about having said something offensive or inappropriate.
Common Compulsions in False Memory OCD
People with false memory OCD often engage in compulsions to try to resolve their doubts. As with all types of OCD, these behaviors can temporarily reduce anxiety but ultimately strengthen the OCD cycle.
These may include:
Reassurance-seeking
Mental checking and rumination
Searching for evidence
Avoidance
Mental neutralization
Confessing
Over-monitoring emotions
Why Trying to “Figure It Out” Makes OCD Worse
One of the most frustrating aspects of false memory OCD is that the urge to solve the doubt actually makes the problem worse. The human brain cannot achieve perfect certainty about the past. Even very clear memories contain gaps and distortions.
When someone with OCD tries to analyze a memory repeatedly, they are essentially trying to solve an unsolvable puzzle. Each mental review introduces new interpretations, emotions, and imagined details. Over time, the memory becomes less stable rather than more accurate.
This creates what many therapists call the rumination trap. The person believes that if they just think about the event long enough, they will finally reach certainty. Instead, the opposite happens. The more they analyze the memory, the more doubt appears.
Breaking this cycle often involves learning to accept uncertainty rather than trying to eliminate it. This concept is closely related to psychological flexibility, which is a central principle in therapies such as ACT.
Effective Treatment for False Memory OCD
False memory OCD can feel overwhelming, but effective treatments are available. Several evidence-based approaches have been shown to help people regain control over obsessive doubt.
Exposure and Response Prevention (ERP)
Exposure and Response Prevention is considered the gold-standard treatment for OCD. In ERP, individuals gradually face the thoughts or situations that trigger their obsessions while resisting the urge to perform compulsions.
Over time, this helps the brain learn that uncertainty can be tolerated without engaging in reassurance-seeking or rumination. For example, someone might practice allowing the thought “Maybe I did something wrong, maybe I didn’t” without trying to mentally review the event.
Cognitive Behavioral Therapy (CBT)
Cognitive Behavioral Therapy helps individuals identify and challenge distorted thinking patterns that contribute to OCD. In false memory OCD, CBT may focus on beliefs such as thought-action fusion or the assumption that memories must be perfectly reliable.
By learning to recognize these cognitive distortions, individuals can begin to reduce the power of obsessive doubt.
Acceptance and Commitment Therapy (ACT)
Acceptance and Commitment Therapy emphasizes psychological flexibility rather than certainty. Instead of trying to eliminate intrusive thoughts, ACT encourages people to observe them with openness and distance.
The goal is to move forward with meaningful actions even when uncertainty remains. This approach can be particularly helpful for false memory OCD, where the core struggle revolves around the impossibility of achieving perfect certainty.
Medication
In some cases, medication may be recommended alongside therapy. Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed for OCD and can help reduce the intensity of obsessive thoughts and anxiety.
Medication decisions should always be made in consultation with a qualified mental health professional.
When to Seek Professional Help
Occasional doubts about memory are normal. However, professional help may be beneficial if intrusive doubts about the past begin to interfere with daily life.
Signs that it may be time to seek help include spending hours reviewing memories, repeatedly seeking reassurance, or avoiding people and situations due to fear of what might have happened.
If these patterns are causing significant distress or disrupting relationships, work, or sleep, speaking with a therapist experienced in OCD treatment can be an important step toward recovery.
FAQs About False Memory OCD
How common is false memory OCD?
False memory OCD appears to be relatively common among people with obsessive-compulsive disorder. According to data from NOCD, 31.9% of their members with OCD reported experiencing this subtype in 2023.
How can I use digital therapy apps to manage false memory OCD?
Several digital therapy apps provide structured exercises based on evidence-based treatments such as CBT and ACT. These tools can help individuals practice mindfulness, cognitive defusion, and exposure exercises. While apps can be a helpful supplement, they are usually most effective when combined with professional therapy.
What is the difference between false memory OCD and real event OCD?
In false memory OCD, the person fears they may have done something wrong but lacks clear evidence that the event occurred. In real event OCD, the obsession focuses on something that actually happened, but the individual becomes trapped in excessive guilt, rumination, or moral analysis about the event.
How does false memory OCD start?
False memory OCD often begins with a moment of uncertainty about a past event. This uncertainty triggers intrusive thoughts, which lead to rumination and compulsive attempts to verify what happened. Over time, the cycle of doubt and checking reinforces itself, making the memory feel increasingly convincing and distressing.
Psychological flexibility is the ability to stay open, aware, and engaged even when uncomfortable thoughts or emotions are present.
It is not about eliminating distress, but about changing how you relate to your inner experiences so they no longer dictate your behavior.
In ACT, psychological flexibility is strengthened through six core processes: acceptance, cognitive defusion, present-moment awareness, self-as-context, values, and committed action.
Higher psychological flexibility is associated with lower levels of anxiety, depression, and distress, and plays an important role in OCD treatment.
Flexibility grows through practice, not perfection: small, values-guided actions taken in the presence of discomfort build lasting change.
Disclaimer: This article is for educational purposes, not medical advice.
What Is Psychological Flexibility?
Mental rigidity is strongly associated with OCD and other mental disorders. When our thinking patterns are unhelpful and we are not able to change them to better adapt to our circumstances, we are being psychologically rigid.
What’s the opposite of mental rigidity? You guessed right: psychological flexibility.
In the landmark book A Liberated Mind, Stephen Hayes, creator of ACT, describes psychological flexibility as follows:
“Psychological flexibility is the ability to feel and think with openness, to attend voluntarily to your experiences of the present moment, and to move your life in directions that are important to you, building habits that allow you to live life in accordance with your values and aspirations.”
Importantly, he adds that psychological flexibility involves not running away from pain but turning towards it “in order to live a life full of meaning and purpose.”
Psychological flexibility is also about being aware of our inner experience (thoughts, emotions, or urges) but not letting it dictate our actions. We choose how to respond to our present circumstances based on the things we value in life, not what we are feeling or thinking at the moment.
Put in another way: being psychologically flexible is acting in ways that serve our long-term values instead of short-term relief. It’s reacting with intention instead of with impulsivity. Ultimately, psychological flexibility helps us move towards what matters, even when doing so makes us feel uncertain or anxious.
Research consistently shows the benefits of higher psychological flexibility. For example, individuals with greater flexibility typically report lower levels of depression, anxiety, and psychological distress during stressful life events according to a study by Masuda et., al published in 2011.
Characteristics of Psychological Flexibility
Being present: Staying connected to what is happening right now instead of getting lost in worries about the future or ruminations about the past. Presence allows us to respond to reality as it is, rather than as our mind imagines it to be.
Openness: Psychological flexibility involves making room for uncomfortable thoughts and emotions without immediately trying to push them away. Openness creates space for choice, even when internal experiences feel intense or unpleasant.
Engaged: Engagement refers to taking action guided by your values, even when it feels uncomfortable. It means participating in your life in ways that reflect what truly matters to you, rather than being driven by avoidance or short-term relief.
Why Is Psychological Flexibility Important?
Psychological flexibility plays a crucial role in learning and growth. When we are open and curious, rather than defensive or avoidant, we are more able to learn from experience, even from failure, discomfort, or uncertainty.
Flexibility also helps us adapt to changing environments. Life is unpredictable, and rigid ways of thinking or behaving impede our adjustment and success. Psychological flexibility allows us to modify our responses as situations change, rather than clinging to strategies that no longer work.
Importantly, psychological flexibility helps us let go of unhelpful patterns of thinking and behavior. Instead of repeatedly engaging in habits that provide short-term relief but long-term suffering, flexibility allows us to experiment with new, more adaptive ways of responding.
Practical Examples of Psychological Flexibility
The following case studies are fictional but illustrate psychological flexibility at work.
Case 1: Not Quitting a Course of Study Even When Facing Doubt
Daniel, a 29-year-old nursing student in Chicago, began questioning whether he was “smart enough” after failing his first pharmacology exam. Instead of dropping out, he acknowledged the self-doubt, met with his professor, joined a study group, and adjusted his schedule. He chose persistence because becoming a nurse aligned with his long-term values.
Case 2: Responding Calming to a Setback
María, a freelance graphic designer in Madrid, lost a major client unexpectedly. Her first impulse was panic and self-criticism. Instead of spiraling, she took a walk, labeled her thoughts as anxiety, and reviewed her finances objectively. Within a week, she updated her portfolio and reached out to three new prospects.
Case 3: Continuing to Engage in Valued Action Even if You Are Not Feeling Your Best
Jamal, a high school teacher in Atlanta, woke up feeling low and unmotivated after a difficult week. Rather than calling in sick out of avoidance, he showed up and focused on delivering one meaningful lesson. He didn’t try to eliminate his mood. He simply chose to act in line with his commitment to his students.
Case 4: Not Letting Strong Emotions Dominate Your Actions
Elena, a 35-year-old marketing manager in Toronto, felt intense anger after receiving critical feedback during a team meeting. Her instinct was to send a defensive email. Instead, she paused, drafted the message without sending it, and revisited it the next morning. She responded thoughtfully, protecting both her reputation and professional relationships.
Psychological Flexibility and OCD
Obsessive-compulsive disorder (OCD) is strongly associated with psychological inflexibility. Individuals with OCD often feel compelled to respond to intrusive thoughts or distressing sensations in rigid, habitual ways (such as performing compulsions or engaging in mental rituals) to reduce anxiety.
The researchers found that OCD symptoms decreased significantly while psychological flexibility increased over the course of treatment. Importantly, higher average levels of psychological flexibility were associated with lower scores on the Yale-Brown Obsessive Compulsive Scale (Y-BOCS). Greater flexibility significantly predicted lower levels of obsessions and compulsions.
These findings highlight that OCD is not just about the presence of intrusive thoughts, but about the rigid ways people respond to them. Increasing psychological flexibility helps loosen these rigid patterns, allowing individuals to relate differently to intrusive thoughts, urges, and anxiety.
What Is Psychological Flexibility in ACT?
In Acceptance and Commitment Therapy (ACT), psychological flexibility is the central goal of treatment. ACT does not aim to eliminate unpleasant thoughts or feelings. Instead, it focuses on changing how we relate to them so that they no longer dominate our behavior.
ACT teaches skills that help individuals stay present, open, and engaged in life while pursuing what matters to them. Psychological flexibility in ACT is about living fully even in the presence of discomfort.
The Core Processes of Becoming More Psychologically Flexible in ACT
Increasing psychological flexibility in ACT involves strengthening six interrelated core processes, often represented in the ACT hexaflex model. These processes are not steps to be completed in sequence. They are interconnected skills that support and reinforce one another.
You can begin working with any of the processes, and growth in one area often enhances the others. For example, improving cognitive defusion can make acceptance easier, and clarifying values can strengthen committed action.
Rather than aiming for perfect “balance,” psychological flexibility develops as you repeatedly practice these processes in real-life situations.
Acceptance: Acceptance involves allowing internal experiences to be present without struggling against them. This reduces the energy spent on avoidance and control.
Cognitive defusion: Defusion helps people see thoughts as mental events rather than literal truths. This creates distance from unhelpful thinking patterns.
Being present: This refers to mindful awareness of the here and now, rather than thinking about the past or future.
Self-as-context: Self-as-context refers to shifting from being entangled with self-stories (“I am a failure,” “I am broken”) to observing those stories from a broader perspective. Instead of defining yourself by thoughts, roles, or past experiences, you learn to notice them as events occurring within awareness.
Values: Clarifying what truly matters to you is an essential part of the process. Values provide direction for meaningful action.
Committed action: ACT teaches you how to set goals that are practical, measurable and aligned with your values.
ACT Techniques That Support Psychological Flexibility
Here are a few ACT techniques to help you become more proficient in every core process.
Look at It as an Object (Defusion): The goal of this exercise is to lessen the impact of troubling thoughts. Pick a thought that’s bothering you and ask yourself: if it had a size, what would it be? If it were an object, what shape would it have? Continue this process with the reactions you have to the thought. After analyzing each reaction in this way, return to the original thought. Does it still feel as heavy or threatening?
Rewriting Your Own Story (Self-as-context): Write a couple hundred words about a situation you’ve struggled with. Then reread what you wrote and circle all words that describe internal reactions (thoughts, feelings, memories, sensations, or behaviors). Next, underline all external situations or facts. Finally (and this is the key step), rewrite the story so that all the circled and underlined elements remain, but the theme, meaning, and direction of the story are completely different.
Open the Door (Acceptance): Rather than trying to push away uncomfortable emotions, you imagine opening the door and allowing them in. You might notice tightness in your chest or a wave of sadness and make room for it instead of fighting it. Acceptance doesn’t mean liking the feeling—it means dropping the struggle so you can move forward.
Broaden and Narrow Your Attention (Presence): The point of this exercise is to train your ability to shift and control your attention. Lie down comfortably and play a song that includes several instruments (e.g., wind, strings, percussion). Focus your attention solely on one instrument, then shift your attention to a different instrument every minute. This deliberate shifting strengthens your capacity to stay present and direct your focus intentionally.
Flipping Pain into Purpose (Values):Difficult emotions often point toward something meaningful. Grief signals love; anxiety signals importance. By identifying the value underneath the pain, you can use discomfort as a compass that guides you toward what truly matters in your life.
SMART Goal Setting (Committed Action): Once you’ve clarified your values, you translate them into specific, measurable, achievable, relevant, and time-bound goals. For example, if connection is a value, you might commit to calling a friend once a week. Small, consistent steps build momentum and reinforce valued living, even when motivation fluctuates.
Other Ways to Improve Psychological Flexibility
Psychological flexibility is a skill that can be developed over time. One simple way to build flexibility is to learn something new every day, even in small ways. Novel experiences challenge rigid thinking patterns and encourage curiosity.
Another helpful practice is changing routines. Small changes (such as taking a different route, trying new foods, or altering daily habits) can gently stretch psychological flexibility and reduce reliance on automatic behavior.
Practicing mindfulness, reflecting on values, and intentionally choosing actions aligned with long-term goals can all contribute to increased psychological flexibility over time.
Psychological Flexibility FAQ
How can I find a coach focusing on psychological flexibility skills?
Look for coaches or therapists trained in Acceptance and Commitment Therapy (ACT) or contextual behavioral approaches. Many professionals explicitly mention psychological flexibility as a core focus of their work.
Which online therapy platforms specialize in psychological flexibility techniques?
The Association for Behavioral and Cognitive Therapies (ABCT) offers a large, searchable database of therapists that can be filtered by specialty, including ACT. It’s Complicated is another helpful platform for finding therapists who specialize in ACT and other evidence-based approaches.
What are the best apps to improve psychological flexibility?
ACT Companion can be a helpful tool for building psychological flexibility. There are also apps that target specific processes. Headspace, for example, focuses on meditation and mindfulness, helping you strengthen present-moment awareness. Clarity: CBT Self-Help Journal can support work on defusion and self-as-context by helping you identify, examine, and reframe unhelpful thought patterns.
What are the three pillars of psychological flexibility?
While models vary, psychological flexibility is often summarized as openness, awareness, and engagement: being open to experience, aware of the present moment, and engaged in valued action.
Real event OCD focuses on the meaning assigned to past events, not the events themselves. The distress comes from how OCD interprets what happened, not from the memory alone.
Guilt and shame are normal emotions that become amplified in real event OCD. Instead of guiding learning or repair, they are used by OCD to question your character and demand certainty.
Compulsions keep real event OCD alive. Mental review, reassurance seeking, and confession provide short-term relief but reinforce the OCD cycle over time.
Recovery involves learning to tolerate uncertainty rather than resolving the past. Evidence-based treatments like ERP and ACT help change your relationship with intrusive thoughts and memories.
You can move toward a meaningful life even while guilt or doubt is present. Progress does not require certainty, forgiveness, or emotional relief.
Disclaimer: This article is for educational purposes, not medical advice.
Real Event OCD: How OCD Interprets The Past
Real event OCD is a form of obsessive-compulsive disorder where the obsessions focus on something that actually happened in the past. Unlike intrusive thoughts that feel hypothetical or irrational, real event OCD latches onto real memories (things you said, did, or failed to do) and convinces you that they reveal something terrible about who you are.
People with real event OCD often replay a past situation endlessly, asking questions like:
What if I seriously hurt someone?
What if that mistake means I’m a bad person?
What if I should still be punished for what I did?
The distress doesn’t come from the event itself so much as from the meaning OCD assigns to it. The mind treats the memory as evidence in a moral trial that never ends.
Real event OCD is especially painful because it attacks values like integrity, kindness, responsibility, and empathy, qualities that matter deeply to the person experiencing it. A person with real event OCD may interpret the event as proof that they are a bad person.
How Real Event OCD Works and How Your Mind Gets Hooked
Real event OCD is best understood as having three interacting components:
The event: something that actually happened in the past.
The obsessions: intrusive thoughts, questions, and interpretations about what the event means.
The compulsions: mental or behavioral efforts to resolve the distress caused by those obsessions. A common compulsion is asking people for reassurance or confessing.
The event itself is not the problem. Many people experience regret or guilt about past actions. What turns a memory into real event OCD is what happens after the event is recalled.
The Role of Guilt and Shame
Guilt and shame are not pathological. Guilt helps us recognize when our actions don’t align with our values. Shame can signal social boundaries and prompt reflection.
In real event OCD, these emotions are amplified and turned against you. Instead of guiding learning or repair, guilt becomes proof of moral danger. Shame becomes identity-based: “If I feel this bad, it must mean something is deeply wrong with me.”
The mind stops asking, “What can I learn?” and starts asking, “What does this say about who I am?”
The Role of Uncertainty
Just like with other OCD subtypes, such as Relationship OCD, real event OCD is fueled by an intolerance of moral uncertainty.
The mind demands impossible answers:
Was my intention bad or just imperfect?
Did I cause harm, or could I have?
Was it forgivable or unforgivable?
These questions have no final resolution, yet OCD insists they must be answered before you can move on. The more you try to solve them through thinking, the more stuck you become.
Cognitive Distortions That Keep Real Event OCD Going
Several faulty thinking patterns make real event OCD feel convincing and inescapable.
Emotional reasoning: “Because I feel intense guilt or shame, the event must have been truly terrible.” Here, emotions are treated as evidence. In reality, OCD can generate intense feelings even when no new information is present.
Magnification: Small or ambiguous actions are blown out of proportion. A brief comment becomes cruel. An awkward moment becomes traumatic. A mistake becomes unforgivable. The event is mentally zoomed in on until it feels catastrophic.
Personalization: Responsibility is exaggerated. You may assume you caused harm without clear evidence or believe you should have predicted outcomes that were unknowable at the time. Neutral or shared situations become framed as solely your fault.
All-or-nothing thinking: Events are judged in extremes. You are either a good person or a bad person. The action was either acceptable or morally damning. There is no room for complexity, growth, or human imperfection.
How the OCD Cycle Locks Everything in Place
Together, these distortions feed the OCD cycle:
A memory arises (event).
Distorted interpretations appear (obsessions).
Guilt and anxiety spike.
Compulsions are performed to gain certainty or relief.
Relief fades, and the memory returns stronger.
Over time, the memory feels more vivid and emotionally charged, not because it’s becoming clearer, but because OCD has trained the brain to treat it as dangerous.
Understanding this process is not about proving innocence. It’s about seeing why thinking harder has never brought peace and why a different approach is needed. It’s about realizing the need to overcome intrusive thoughts without fighting them.
Examples of Real Event OCD
Replaying a conversation from years ago and fearing you were emotionally abusive.
Obsessing over a joke you made and worrying it caused lasting harm.
Fixating on a mistake at work and believing it proves you are unethical.
Ruminating over a moment of anger and fearing it reveals violent intent.
Re-examining a past relationship and questioning whether you manipulated the other person.
Obsessing over something you didn’t say or do and believing that omission caused serious damage.
Ruminating over a past sexual encounter and fearing your behavior was abusive, harmful, or non-consensual.
Real Event OCD vs Typical Guilt or Regret
Everyone experiences guilt or regret at times. The difference lies in intensity, rigidity, and function. Healthy guilt is proportionate. It rises, delivers its message, and fades. It often leads to constructive action such as apologizing, making amends, or adjusting future behavior.
Real event OCD, on the other hand, is sticky and relentless. It doesn’t resolve. It demands certainty about the past and your moral character, long after any useful lesson has been learned.
Normal Guilt or Regret
Real Event OCD
Proportionate to the situation.
Feels excessive, overwhelming, or out of proportion.
Arises, delivers information, and naturally fades.
Feels sticky and persistent, often lasting months or years.
Focuses on a specific behavior or choice.
Expands to question your character or identity.
Leads to constructive action (e.g., apologizing, repairing, adjusting future behavior).
Leads to mental rumination, self-judgment, and repeated analysis.
Accepts that some uncertainty about the past is unavoidable.
Demands certainty about intentions, impact, or moral meaning.
Allows learning and then movement forward.
Keeps you stuck reviewing the same event repeatedly.
Does not require constant mental checking.
Feels urgent and impossible to “let go” without resolution.
Supports growth and value-aligned behavior.
Interferes with daily life and pulls attention away from the present.
Real Event OCD vs False Memory OCD
Real event OCD and false memory OCD can look similar, but they differ in a key way.
Real event OCD focuses on events that truly occurred, even if details are exaggerated or distorted by anxiety. False memory OCD, on the other hand, centers on fears that something terrible happened despite little or no evidence that it did.
Both involve doubt, rumination, and mental review. Both attack a person’s sense of self. And both are maintained by compulsive attempts to achieve certainty. Importantly, treatment for both follows the same principles: ERP, response prevention, and learning to tolerate uncertainty rather than trying to resolve it.
What Compulsions Are Common in Real Event OCD?
Compulsions in real event OCD are often subtle and mental, which makes them hard to recognize.
Common compulsions include:
Replaying the memory repeatedly to “get it right.”
Analyzing your intentions, tone, or facial expressions.
Mentally arguing with yourself about whether you’re a good person.
Seeking reassurance from others about whether what you did was “that bad.”
Googling moral rules, laws, or ethical standards.
Confessing past actions excessively or repeatedly.
Comparing yourself to others to assess how bad your behavior was.
These behaviors feel necessary, but they keep the OCD cycle alive.
How Is Real Event OCD Treated?
The gold-standard treatment for real event OCD is Exposure and Response Prevention (ERP). ERP doesn’t aim to prove that you’re innocent, forgiven, or morally acceptable. Instead, it helps you learn something more powerful
“you can live a meaningful life without resolving every doubt about the past.”
ERP works by intentionally triggering the obsession (exposure) while refraining from compulsions (response prevention). Over time, the brain learns that the memory is not dangerous and does not require endless analysis.
Examples of Exposures to Treat Real Event OCD
Exposures are tailored to the individual, but common examples include:
Writing out a factual narrative of the event without adding justifications or defenses.
Reading statements like, “I may have hurt someone, and I may never know for sure.”
Imagining the worst-case interpretation of the event without trying to neutralize it.
Allowing the memory to be present while continuing daily activities.
Sitting with feelings of guilt or shame without trying to make them go away.
The goal is not emotional relief but emotional tolerance.
Examples of Response Prevention
Response prevention means resisting the urge to “fix” the feeling.
Examples include:
Not mentally reviewing the event after it arises.
Avoiding reassurance-seeking conversations.
Letting questions like “What does this say about me?” remain unanswered.
Not checking your memory for emotional certainty.
Refraining from self-punishment or mental self-attack.
This can feel deeply uncomfortable at first. That discomfort is part of the healing process.
Through mindfulness practices, ACT helps you notice thoughts like “I am unforgivable.” You can then classify these thoughts as mental events rather than truths that require action. In other words, you can “de-fuse” from the thoughts, giving yourself more room to focus on what actually matters in your life.
ACT also focuses on acceptance, helping you make room for uncomfortable thoughts while choosing behaviors aligned with your values. Ultimately, ACT is all about shifting the focus from “Am I a good person?” to “How do I want to live today?” even with uncertainty, guilt, or doubt present.
Self-Compassion and Real Event OCD
Self-compassion is not about excusing behavior or minimizing harm. In real event OCD, it’s about recognizing shared humanity. Everyone makes mistakes. Everyone causes harm at times. OCD convinces you that your mistakes are uniquely damning.
Practicing self-compassion might involve:
Speaking to yourself as you would to someone you love.
Acknowledging pain without adding self-punishment.
Allowing growth without demanding perfection.
Self-compassion reduces shame, which weakens OCD’s grip.
When Should I Seek Help?
You may want to seek professional help if:
You spend hours a day replaying past events.
Guilt or shame feels overwhelming or constant.
You avoid people, situations, or goals because of the memory.
You feel stuck trying to “figure it out” mentally.
OCD is highly treatable, but it rarely resolves through insight alone. Working with a therapist trained in ERP and ACT can make a significant difference.
Real Event OCD Recovery Stories
The following are real stories from the OCD subreddit and other mental health subreddits shared by people who experienced real event OCD and reported meaningful improvement over time. They are meant to provide hope and guidance, but always keep in mind that what worked for one person may not work for everyone.
Case 1: Medication + Reassurance Avoidance + ERP
Reddit user darkkoffeekitty shared that he was able to make significant progress with real event OCD through a combination of medication and specialized therapy. After several months of intense distress, he noticed a shift after starting Anafranil and working with an OCD therapist.
“Now I wake up every day with pretty much no guilt and reduced anxiety,” he says.
Importantly, he emphasizes the role of reducing compulsions, particularly reassurance seeking and confessional behaviors. He notes that continuing these behaviors only deepened his distress because “you will remember more details or ask more questions about the obsession that will put you in the same pit of despair.”
Case 2: Patience + Consistent Work + Accepting Uncertainty
Another anonymous Reddit user said he now experiences long periods of calm after putting in some work. He regularly listens to OCD-related podcasts like The OCD Stories and Fearcast and reads articles from Dr. Michael J. Greenberg and other clinicians. “I try to work [Dr. Greenberg’s] process, accept uncertainty, and if something does come up in the future I will figure it out then.”
Case 3: Lifestyle Changes + Learning + Letting Go of Perfectionism
A third anonymous Reddit user shared that he had struggled with real event OCD for over two years but experienced noticeable improvement after learning more about the condition and reading about others with similar experiences.
“Being able to see the writing by people who can completely relate to my struggle really helped me,” he says. Reading these accounts helped him realize he was not alone and that others faced the same patterns of doubt, guilt, and rumination.
He also described how perfectionism played a central role in maintaining his anxiety. Much of his distress came from a constant need to be the perfect student and preserve his reputation.
“I just had to realize I can be imperfect, I don’t have to define myself by how perfect I am. I can just be myself.”
He further emphasized moving away from rigid moral categories, noting that many situations cannot be cleanly labeled as “good” or “bad” and often exist in a gray area. In addition, he found that developing healthier routines, such as exercising regularly, made a meaningful difference in his overall well-being.
His final advice focused on taking active steps rather than remaining stuck in rumination:
“Be proactive in searching for ways to help with your OCD. Don’t let yourself sit there and constantly obsess and ruminate. Try to look online, talk to a therapist, or do something to find what works for you.”
What Is Real Event OCD FAQ
What does real event OCD feel like?
Real event OCD often feels like being trapped in a moral courtroom inside your own mind. The memory feels urgent, emotionally charged, and impossible to let go of. Even when others reassure you, the relief is short-lived. The distress comes not from the event alone, but from the endless need to understand, judge, and resolve it with certainty.
Does real event OCD go away?
Yes, real event OCD can improve significantly with proper treatment. While memories don’t disappear, their emotional power and urgency can fade. With ERP and ACT, many people learn to relate to past events without constant rumination, guilt, or self-punishment. Recovery doesn’t mean certainty. It means freedom from the OCD cycle.
Where can I find online therapy services specializing in real event OCD?
Look for therapists or platforms that explicitly mention ERP for OCD and experience with moral or guilt-based obsessions. Many licensed therapists offer online sessions across regions. It’s important to ask directly about OCD-specific training, as general talk therapy alone may unintentionally reinforce rumination.
Are there wearable devices that help track anxiety related to real event OCD?
Some wearable devices can track physiological markers like heart rate variability or sleep patterns, which may help you notice stress trends. However, they do not treat OCD itself. For some people, tracking can become another form of reassurance-seeking. These tools are best used cautiously and alongside evidence-based therapy.
Disclaimer: This article is for educational purposes, not medical advice.
What Are Intrusive Thoughts?
Intrusive thoughts are unwanted thoughts, images, or urges that show up suddenly and feel disturbing, confusing, or alarming. According to the Anxiety and Depression Association of America, six million Americans have intrusive thoughts.
Everyone has strange or uncomfortable thoughts from time to time, but intrusive thoughts feel different from normal worry. They tend to be more intense, more repetitive, and much harder to ignore.
A key difference is how we respond to them. Regular worries don’t hook us. Intrusive thoughts, on the other hand, pull us into the OCD cycle: a thought appears, anxiety spikes, we try to get rid of it, and that effort makes the thought come back stronger. The more energy we use to fight, suppress, or analyze the thought, the more “sticky” it becomes.
Why do we engage with intrusive thoughts so much? Often, rumination becomes a compulsion. We try to fix a problem using the wrong tools: analyzing, neutralizing, or seeking certainty about something that can’t be solved through thinking. While intrusive thoughts can be associated with conditions like OCD or PTSD, many people experience them without having a mental health disorder at all.
Common Types of Intrusive Thoughts
Intrusive thoughts are often ego-dystonic, meaning they go against your values, identity, or desires. People may experience repetitive doubts about deeply important topics like relationships, morality, religion, or identity (e.g., relationship OCD). The content often targets what you care about most.
Common themes include sexual thoughts, violent images, identity doubts, religious fears, relationship doubts, death, and existential questions. Many people fear they might act on these thoughts (e.g., harm OCD), or that the thought itself says something terrible about who they are. A common myth is that “if you think it, you must secretly want it,” which is simply not true.
Identifying Intrusive Thoughts
So how can you tell whether a thought is intrusive?
Intrusive thoughts tend to feel unusual or out of character: They don’t align with your values, intentions, or sense of self. People often say, “This doesn’t feel like me,” or “Why would my brain even go there?”
Intrusive thoughts are bothersome: Intrusive thoughts trigger distress, anxiety, guilt, or shame. Even if the content seems irrational, the emotional reaction feels very real. The distress isn’t about curiosity or reflection; it’s about fear and urgency.
Intrusive thoughts are hard to control: Trying to suppress them often backfires. The more you tell yourself “don’t think this,” the louder and more frequent the thought becomes. This loss of control is frustrating and often leads to increased monitoring of your mind, which keeps the cycle going.
If a thought feels sticky, distressing, repetitive, and resistant to logic or reassurance, there’s a good chance you’re dealing with an intrusive thought rather than a meaningful signal or intuition.
Should I Worry About My Intrusive Thoughts?
In short: no. Intrusive thoughts are not impulses. People who experience them are not at higher risk of acting on them. In fact, the issue is usually over-control, not lack of control. You care deeply about preventing harm, which is why the thoughts feel so disturbing.
Take harm OCD as an example. One common theme within this subtype involves obsessive fears about becoming a serial killer. These fears arise precisely because not harming others is a deeply held value, making the thought of committing violence feel unbearable and deeply distressing. However, as NOCD explains, people with harm OCD are no more likely than the general population to harm someone. In fact, they may be even less likely, given how vigilant they are about these thoughts and how much distress the thoughts cause them.
That being said, you might consider seeing a therapist if intrusive thoughts are causing significant distress, taking up a lot of mental space, leading to compulsive behaviors, or interfering with daily life. A therapist trained in OCD-informed approaches can help you change your relationship with these thoughts rather than trying to eliminate them.
How to Stop Intrusive Thoughts: Give Up Fighting
This may sound counterintuitive, but the most effective way to deal with intrusive thoughts is to stop fighting them.
There’s solid psychological science behind this. In an article published in Behaviour Research and Therapy, researchers found that thought suppression is counterproductive, while acceptance is a more effective technique.
A common metaphor used in ACT is the Chinese finger trap: the harder you pull to escape, the tighter it grips. Relief comes from gently moving inward, not forcing your way out.
The Chinese finger trap metaphor shows how struggling against intrusive thoughts can make them feel more stuck.
The goal isn’t to make thoughts disappear. It’s to develop a new relationship with them. Instead of treating thoughts as threats that must be analyzed or neutralized, you learn to see them as mental events that can come and go on their own.
“The central shift is from a focus on what you think and feel to how do you relate to what you think and feel”
Steven C. Hayes, A Liberated Mind
Traditional CBT (Cognitive Behavioral Therapy) helps by identifying unhelpful thinking patterns and reducing reassurance and compulsions. ACT (Acceptance and Commitment Therapy) builds on this by emphasizing defusion (creating distance from thoughts) and acceptance (allowing internal experiences without resistance). Together, these approaches help loosen the grip intrusive thoughts have over your attention and emotions.
What Exercises Are Good for Intrusive Thoughts?
Acknowledge the thought: Gently notice the thought without judging it or trying to push it away. A simple “I’m noticing an intrusive thought” can interrupt the automatic struggle.
Give your brain a name and politely agree with it: This ACT exercise might sound strange, but it’s powerful. You might say, “Thanks, Kyle, I see you’re trying to protect me,” without debating or correcting the content.
Mindfulness: Mindfulness helps you observe thoughts rather than get pulled into them. Simple practices include focusing on the breath, noticing sounds in the room, or doing a brief body scan for one to two minutes.
Redirect attention to physical sensations: Bring attention to your feet on the floor, the feeling of your hands, or your breathing. This grounds you in the present moment without trying to escape the thought.
Give shape and color to the thought: Visualize the thought as an object, cloud, or cartoon image. This creates distance and reminds you that thoughts are experiences, not commands or truths.
Avoid reassurance: Reassurance feels helpful short-term but keeps the cycle alive. Each time you seek certainty, you teach your brain that the thought was dangerous.
Open the door: Imagine opening a door and allowing uncomfortable thoughts and feelings to enter and leave freely. You “accept” these unwanted visitors and allow them to leave of their own accord.
Drop the rope: Picture a tug-of-war between you and the thought. Now picture yourself dropping the rope and shifting your attention instead to the things that matter in your life. You are no longer engaged in this senseless game, so you can actually focus on the things that are meaningful to you.
Stop Intrusive Thoughts Without Fighting FAQ
How can I use mobile apps to manage intrusive thoughts?
Apps that focus on mindfulness, acceptance, or cognitive defusion can be helpful when used gently. Avoid apps that encourage constant monitoring or reassurance.
How to find a therapist specializing in obsessive thoughts near me?
Look for therapists trained in CBT or ACT with experience treating OCD. International clinics, expat health networks, and online directories can be good starting points.
Where can I find support groups for anxiety and disturbing thoughts locally?
Local mental health clinics or expat communities sometimes host support groups. Online groups can also be helpful if local options are limited.
Does having intrusive thoughts mean I have OCD or some other mental condition?
Not necessarily. Intrusive thoughts are extremely common. A diagnosis depends on how much distress they cause and whether compulsive behaviors are present.